
– to fit the many skeletons in the closet of the official Corona narrative:
Our critique of Watson et al’s modelling study is published – Vaccine side effects, unexplained deaths demand clarification
Occasionally I sing the “Dichterliebe”. This is the song cycle that Robert Schumann set to music based on poems by German poet Heinrich Heine. In it, Heine came to terms with his unhappy love. In the last song, No. 16, (here in a very beautiful recording, with Fritz Wunderlich), the poet sings:
The old evil songs,
the dreams evil and bad,
Heinrich Heine
Let us bury them now,
get a big coffin.
Into it I put many a thing,
yet I say not yet what.
The coffin must be even bigger
than a Heidelberg barrel…
I felt reminded of this several times these days, trying to find out if Covid-19 vaccinations have prevented deaths, and seeing the plethora of information slowly oozing out of all corners: Excess mortality, deaths, severe vaccine side effects. Even the world’s vaccination champion Gates now admits that it all didn’t work out as planned after all.
I want to address such questions in this blog. First, I address our new analysis on that model by the Imperial College working group of Watson and others [1]. Our analysis just became available online [2]. And then I discuss some recent information on the issue of side effects and excess mortality despite or because of vaccinations.
Our critique of the Watson model, which claims Covid-19 vaccines saved 16 million lives
I reviewed the study by Watson and colleagues once before, when it was published in August 2022. I’ll briefly remind you: the research group from Imperial College London presented a mathematical modelling study that calculated that the Covid-19 vaccinations saved 16-20 million people’s lives.
The leader of this working group is mathematician Neil Ferguson, who published the first predictive model in March 2020 [3], with wild calculations that were all enormously off, not because we did the lockdown he called for, but because the models are simply unusable. The RKI (German government agency responsible for disease control and prevention) had also adopted this model [4].
Now we have published a formal and relatively detailed critique of this Watson model, which is available as a peer-reviewed preprint on the journal page of the journal “Futures” [2]. We embed our critique in a basic critique of such models. But in brief and simple terms, the critique has the following core:
The model of Watson and colleagues uses a double modelling approach. First, it takes modelled data as its basis, namely the data calculated by an excess mortality model published by The Economist magazine up to December 2021. With this and the Covid-19 mortality data from the Covid dashboards, it now feeds its own mathematical model. Since the current Covid-19 mortality data has the effects of vaccination built in, so to speak, theoretically, if you fitted the model and ran on the earlier excess mortality data from The Economist model, leaving all other parameters, e.g. the virus reproduction number, the same, you could derive a counterfactual model. This would give you a reality that would have been different. The difference between the models would then give the number of lives saved. That’s about 16 to 20 million.
So much, in essence, about the analysis by Watson and colleagues. The publication in the journal Lancet Infectious Diseases made it very visible. Thus, apparently, truthfulness is vouched for and sealed. But one does not have to dig very deep to see how unsteady the whole model stands.
We point out a few technical points in our article, which I’ll skip now. The two main criticisms that make the model completely unusable are as follows:
For one thing, the data the models use is insufficient. I pointed out in my blog on a preprint by Rockenfeller and colleagues[5] the importance of the length of the time series from which one estimates excess mortality. In models such as the Economist model, Euromomo, or that of the WHO, the excess mortality estimate is obtained from a few years ahead. Rockenfeller and colleagues have used 20 years of data for model fitting and were able to show that the commonly used models provide a gross overestimation of the mortality than can really be expected. Therefore, it is not at all factually admissible to use the data of the Economist model. They are not stable and factually incorrect. The analysis by Rockenfeller and colleagues shows this very clearly, using Germany as an example.
The Watson model was also calibrated on real Covid-19 mortality data. But even these are far from reliable. How fundamentally wrong the model is can be seen from the fact that the underlying mathematical model [6] predicted about 419,000 Covid-19 deaths for Germany as of April 2021, while for Uganda the model predicted about 320,000 deaths. However, according to “Our World in Data – OWID“, there were 82,850 Covid-19 deaths in Germany by that date and 342 in Uganda. The large discrepancy could not have been due to vaccination. Because at that time in Germany just under 8% were vaccinated and in Uganda probably even less. Even if one cannot assume the same reporting logistics for Africa as for Germany, it is difficult to justify the figure overestimated in Uganda by a factor of 9,300 with African conditions and the figure overestimated in Germany by a factor of 5 with a lack of German thoroughness. No, the figures simply show: the model is fundamentally wrong.
Why? We come to that in other parts of our critique: It leaves out far too many factors that matter. And that’s basically true of all these epidemiological models. Resistance factors, host factors, protective factors are left out. Other factors that contributed to mortality are not taken into account, such as incorrect treatments, secondary effects of lockdown, misattribution of deaths to viral disease and much more.
The models also work with an overestimated infection-fatality rate (IFR) by a factor of 3-10, i.e. the ratio of deceased to sick. However, this figure enters into the calculations and with a simple arithmetic reformulation, which we show, one can see that the effectiveness of the vaccine is overestimated if the IFR is set too high. Since the IFR depends on the case definition, which in turn depends, among other things, on the frequency of PCR testing, but also on how many silent, asymptomatic infections there have been, this is a critical parameter. Ioannidis has often pointed out that this figure is overestimated [7-9].
Furthermore, a minor technical side note, the models treat the reproduction number R of the virus as if it were a constant. This is simply wrong. Because it is not a constant, it is a dynamic value, technically it is a data point that would have to be predicted by the models or entered as a dynamic model parameter.
But our very basic critique of these models goes even deeper. They are the spawn of a mechanistic, one-dimensional way of thinking. They only take into account the viruses as the sole actors in the world of the pandemic. Everything depends on their infectivity. Everything else is ignored. But we humans are not just billiard balls on a billiard table with which the evil viruses play. Rather, we are in multiple dependencies that protect or threaten us. We can strengthen our immunological resistance through our behaviour, through protective factors such as exercise, air, sunshine, vitamin D, relaxation, social contacts, connectedness, and weaken it through fear, stress, lack of sleep, and behaviour that is detrimental to our health. This is a foundational critique that criticizes this limited approach, that is, the very premise of knowledge.
There are counter-examples [10, 11]. These models are ones that try to capture the many causal processes that drive events. They are many times more complex, constantly adapting based on new evidence and data, and therefore less susceptible to flawed old data.
It is actually astonishing that such a weak publication as that of Watson and colleagues found its way into one of the important journals. We suspect: financial conflicts of interest. After all, the working group is funded by the vaccination alliance GAVI and by the Bill and Melinda Gates Foundation, which incidentally fund the Lancet Journals.
We formulated the core of our critique soon after the Watson article appeared and sent it to Lancet itself as well as to a number of other journals, all of which waved it off. The content were of no interest to anyone, it were outdated, the journal did not care about criticism of other journals’ publications, and all kinds of other arguments for rejection. The reviewers of Futures encouraged us to include our critique in an epistemological discussion, so the title comes across as unwieldy and the text a bit lengthy.
But the message should be clear: The claim that vaccinations have saved lives, and millions at that, is false. We show why: the underlying numbers are wrong. The mathematical model is too simplistic. And the presuppositions of the entire model are useless.
Adverse effects and excess mortality after the vaccination campaign
Meanwhile, reports of side effects from these vaccinations are piling up. Not that this is new. But what is new now is the fact that this information is increasingly finding its way into conventional news channels.
The Hippocratic Oath Medical Association”, for example, points out that this vaccination is affecting the fertility of young people, that excess mortality in 2021 and 2022 is most likely related to vaccination, and that cancer incidence is increasing. Therefore, the association calls on churches, officials and politicians to stop these vaccinations immediately. It also calls for accountability of those responsible and their immediate dismissal. Our good Dr. Wieler (Head of the RKI during the pandemic) has smelled a rat and has already sought the far in time. But the doctors are also calling for a commission of enquiry and a judicial review.
Uwe Kranz, a former police chief (ret.) who helped set up Europol, is also calling for consequences, describing in one interview the supermortality and in another the vaccination side effects.
Dear colleagues from the press, radio and television (PRT):
Maybe listen to the message itself for a change, instead of first looking to see who the messenger is and then taking the precaution of beating him up in the hope that he might then shut up!
Because this fad of either beating up or ignoring the messenger because he doesn’t have the right clothes on and doesn’t bring the right stable smell, that’s exactly what has led us into this dilemma. Many predicted this problem. No one listened.
The epidemic of those who suddenly died young
I read a moving book at the weekend, Ed Dowd “Cause Unknown” – The epidemic of sudden deaths 2021/2022″ [12]. No, dear PRT members, this is not a conspiracy book just because it was published by Skyhorse. It is backed up with facts. It is also a tear-jerker. Because it documents, with illustrated newspaper reports, usually 6 per page over many pages, published death reports of young sportsmen, athletes or people who collapsed “suddenly, unexpectedly and completely healthy”, “with no apparent previous illness”. The reports are marked with QR codes so that the newspaper reports can be checked. The back pages document 550 such cases. There has never been anything like this before.
Ed Dowd is a Wall Street analyst who worked for Blackrock, one of the world’s largest asset managers [13], where he grew the portfolio he managed by 12 billion in the ten years he was there. He achieved this because he was good at spotting trends before others saw them. This ability also helped him see the turnaround in mortality statistics.
He founded his own company and within the company a Humanity Project, with which he analyses excess mortality. For Germany, the analyses for the 40-49 age group look like this (Figures 1 and 2).
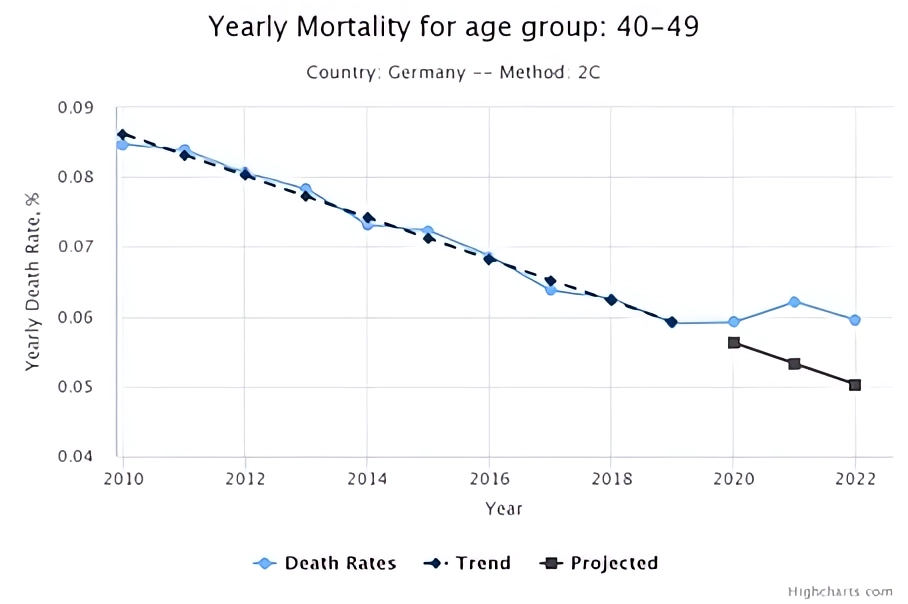
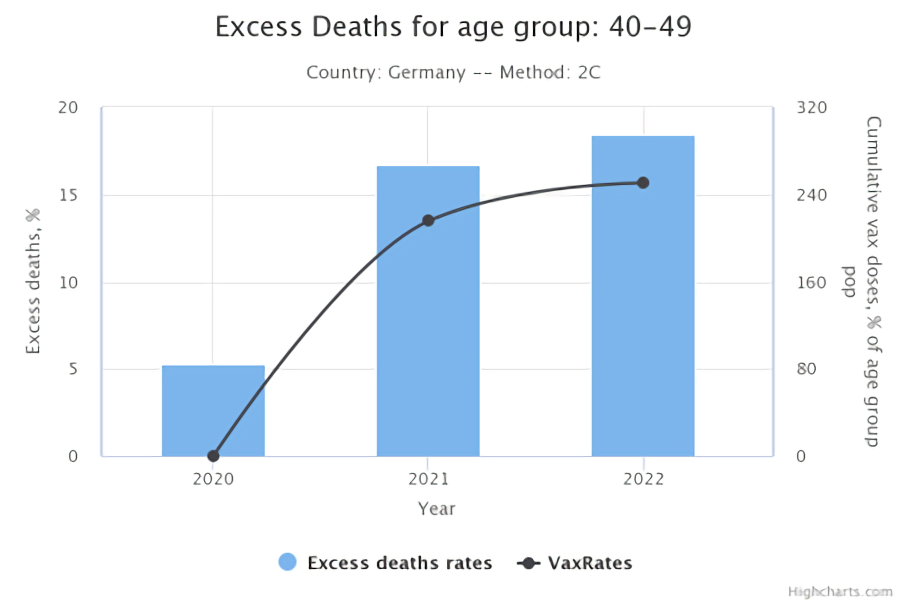
It is informative to study the data and graphs on this website; there you can call up different countries and within countries different age groups. They are constantly adjusted to the data, and they all have a simple, clear and frightening message, which Dowd also expresses in his book: it is mainly the young, healthy, fit and sporty people who are dying now, and much more than one would expect. The data Dowd uses to back up his argument in the book are those that can be found on his website. There is also a very detailed document there describing the methodology.
Now ladies and gentlemen of PRT, dear science editors: What does it tell us when the smartest financiers in the world, who serve or have served the richest and most powerful people in the world to increase their wealth by double-digit percentages, when these people suddenly put their money and brainpower into producing such data that really our public offices, our government agencies, and, yes, really you too, should have produced long ago?
What does this tell us, ladies and gentlemen of the public health agencies, of the committees of the parliaments, of the working groups of our parties, when you, together with our leading media, still try to tread softly and dismiss such data with the commonplace argument that these are only correlations? That’s right. They are correlations. But strong correlations that one does not expect, namely a strong increase in death rates, especially among young people, in parallel with the administration of a new medical technology that is euphemistically declared as “vaccination”. This demands explanation. I have yet to hear any other clever explanation that would explain this correlation in a reasonable, insightful and factually comprehensible way.
Workshop report
I myself am in the process of trying to understand whether one can document this relationship using a time series analysis, in this case an ARIMA analysis. I fitted a time series to the Covid-19 mortality data in Germany and used an intervention term at the beginning of the vaccination campaign. It was significant and relatively clear. And it was positive. That is, vaccination would worsen Covid-19 mortality if this analysis is correct. The impact on ICU bed occupancy was not apparent. These are preliminary analyses that I don’t think are robust. The reason I say this here is that I would urge competent colleagues who may be reading this to contact me to verify, refute or improve this analysis. I am happy to provide my analysis report and data.
The English data on lack of efficacy and a rapid risk-benefit assessment
In England, at least, data are being published from which one can derive a risk-benefit analysis. On January 23rd, 2023, the Joint Committee on Vaccinations published a report. You have to check the appendix to see the explosive nature.
Then you see: In the middle age groups, the risk of Covid-19 hospitalization increases with the number of vaccinations. So, the more vaccinated, the higher the risk of being hospitalized with a Covid-19 diagnosis. While unvaccinated people aged 40-49 have 14.5 hospitalizations per million people, those with one or two doses have 20.1. For subsequent age cohorts, the risk of Covid-19 hospitalization is also higher with than without vaccination. The same is true for severe hospitalization in the middle age groups. It is not much different in the younger groups. Only among the very old is there a positive effect. The Number Needed to Vaccinate (NNV), i.e. the number of people who need to be vaccinated to prevent a case of hospitalization, is between 19,000 and 54,000 people in the middle-aged group and increases to between 48,000 and 176,000 people with booster vaccinations. For younger people, the NNV is always above 100,000 and goes up almost to 500,000 for some age groups.
The NNV for deaths is no longer given at all. I wonder why. Because vaccination most likely does not prevent deaths at all. At the time [14-16] we had estimated a rough NNV of 12,000 – 25,000 to prevent one death and got flogged for it. Now it turns out that this estimate was most likely far too kind. After all, one has to put these numbers in relation to the expected side effects. According to the analysis of regulatory data that Fraiman and colleagues studied [17], the incidence of serious adverse events ranges from 15 to 10 per 10,000, or 150 to 100 per 100,000, depending on the vaccine. So we vaccinate anything from 5,000 to 400,000 people to prevent one case, in numbers:1 case of serious hospitalization with Covid-19. If we do that, we’re taking anything between 7 and 600 serious adverse events to prevent that one case of hospitalization. This risk-benefit ratio is so perversely negative that even the Vaccination Commission in England could only hide it without comment in an appendix table. If you don’t believe it, Dr. John Campbell explains it well in half an hour.
“Quo usque tandem, Catilina, abutere patientia nostra – How long, Catilina, will you abuse our patience”. This is how Cicero introduced his invective against Catilina, the republican conspirator, which eventually led to a suppression of his revolt, if I remember my Roman history correctly. The same could be exclaimed today: How much longer must it be before anyone with enough power and influence has the courage to break the silence? What is happening here is unspeakable. It is wrong. It is ethically wrong. It is factually wrong. It is unreasonable in the extreme. It was an attack on physical integrity, and it was an insult to reason (that’s the least of it, I think). I find it appalling how many put up with it and don’t cry out loud. I find it unbearable that all of our leaders look the other way. I find it deeply disturbing how our entire leading media landscape, apart from small fig-leaf exceptions, has continued to pray the fairy tale of the need for vaccination for a full 3 years.
And here you are still getting excited, dear fact checkers and media makers of PRT, that some people see a conspiracy at work? Yes, how else can such lunacy be explained except by intent, exorbitant cowardice, or colossal irrationality and incompetence on the part of key decision-makers? And which of these would be worse? Or can anyone give me a better explanation?
Sources and literature
- Watson OJ, Barnsley G, Toor J, Hogan AB, Winskill P, Ghani AC. Global impact of the first year of COVID-19 vaccination: a mathematical modelling study. Lancet Infectious Diseases. 2022. doi: https://doi.org/10.1016/S1473-3099(22)00320-6.
- Klement RJ, Walach H. SEIR models in the light of Critical Realism – a critique of exaggerated claims about the effectiveness of Covid 19 vaccinations Futures. 2023;accepted.
- Ferguson N, Laydon D, Nedjati Gilani G, Imai N, Ainslie K, Baguelin M, et al. Impact of non-pharmaceutical interventions (NPIs) to reduce COVID19 mortality and healthcare demand. London: Imperial College, 2020.
- an der Heiden M, Buchholz U. Modellierung von Beispielszenarien der SARS-CoV-2-Epidemie 2020 in Deutschland. Berlin: Robert Koch Institut, 2020.
- Rockenfeller R, Günther M, Mörl F. Reports of deaths are an exaggeration: German (PCR-test-positive) fatality counts during the SARS-CoV-2 era in the context of all-cause mortality. MeRxiv. 2022;https://doi.org/10.1101/2022.11.18.22282534
- Walker PGT, Whittaker C, Watson OJ, Baguelin M, Winskill P, Hamlet A, et al. The impact of COVID-19 and strategies for mitigation and suppression in low- and middle-income countries. Science. 2020;369(6502):413-22. doi: https://doi.org/10.1126/science.abc0035.
- Ioannidis JPA. The infection fatality rate of COVID-19 inferred from seroprevalence data. Bulletin of the World Health Organization. 2021;99:19-33F. doi: https://doi.org/10.2471/BLT.20.265892.
- Ioannidis JPA. Reconciling estimates of global spread and infection fatality rates of COVID-19: an overview of systematic evaluations. European Journal of Clinical Investigation. 2021;51:e13554. doi: https://doi.org/10.1111/eci.13554.
- Axfors C, Ioannidis JPA. Infection fatality rate of COVID-19 in community-dwelling populations with emphasis on the elderly: An overview. medRxiv. 2021:2021.07.08.21260210. doi: https://doi.org/10.1101/2021.07.08.21260210.
- Friston KJ, Parr T, Zeidman P, Razi A, Flandin G, Daunizeau J, et al. Tracking and tracing in the UK: a dynamic causal modelling study. arXiv. 2020;2005.07994.
- Friston KJ, Parr T, Zeidman P, Razi A, Flandin G, Daunizeau J, et al. Second waves, social distancing, and the spread of COVID-19 across America. Wellcome Open Res 5(103). 2021. doi: https://doi.org/10.12688/wellcomeopenres.15986.3.
- Dowd E. “Cause Unknown” – The epidemic of Sudden Deaths in 2021 and 2022. New York: Skyhorse; 2022.
- Rügemer W. Blackrock und Co enteignen. Frankfurt: Nomen; 2021.
- Walach H, Klement RJ, Aukema W. Retracted: The Safety of COVID-19 Vaccinations—We Should Rethink the Policy. Vaccines. 2021;9(7):693. doi: 10.3390/vaccines9070693. PubMed PMID: doi: https://doi.org/10.3390/vaccines9070693.
- Walach H, Klement RJ, Aukema W. The risk-benefit ratio of Covid-19 vaccines: Publication policy by retraction does nothing to improve it. Clinical and Translational Discovery. 2022;2(1):e35. doi: https://doi.org/10.1002/ctd2.35.
- Walach H, Klement RJ, Aukema W. The Safety of COVID-19 Vaccinations — Should We Rethink the Policy? Science, Public Health Policy, and the Law. 2021;3:87-99. https://www.publichealthpolicyjournal.com/general-5.
- Fraiman J, Erviti J, Jones M, Greenland S, Whelan P, Kaplan RM, et al. Serious adverse events of special interest following mRNA COVID-19 vaccination in randomized trials in adults. Vaccine. 2022;40(40):5798-805. doi: https://doi.org/10.1016/j.vaccine.2022.08.036.