
The Pfizer pivotal study is compromised and unreliable
A new paper in the British Medical Journal reveals that and how the Pfizer trial that led to the approval of the BioNTech vaccine was compromised [1]. Paul Thacker, an investigative journalist, reports on a whistleblower, Brook Jackson, who worked at one of the clinical centres, Ventavia in Texas. Ventavia is one of the largest clinical research service providers in Texas and was one of the companies that organized patients for the clinical trial and managed their data. These were “only” 1,000 of the approximately 53,000 patients, but the reported conditions speak volumes. For Jackson had repeatedly pointed out to the company management errors in implementation, poor data quality, patients whose complaints were not followed up, side effects that were not neatly registered, unblinding and any number of other problems.
It’s worth reading in the original. The bad thing is: Jackson had brought this to the attention of the US regulatory authority, the FDA. The FDA had neither replied nor pointed out the problems in its approval report. Instead, the whistleblower was dismissed without notice on the very day she reported the matter to the FDA. Research by the journalist shows that other employees who wished to remain anonymous confirmed the statements.
The FDA, we have known for a long time, is funded as an agency by the pharmaceutical companies, which in itself is a scandal [2]. Since this is the case, it handles the companies with kid gloves and serves mainly their interests, no longer the interests of the patients. As a result, only about 1% of the studies that are submitted are audited, i.e. carefully reviewed, and usually only on paper and not in reality. Ventavia, the company in question, was obviously very afraid that such an audit might come. The worries were unnecessary; for the FDA has neither the staff nor the will to look more closely.
Adverse drug reactions are not adequately investigated and documented
On Nov. 2, US Senator Ron Johnson held a hearing with people who have suffered severe side effects due to Covid-19 vaccinations. I don’t usually watch YouTube videos, but I watched these 9 minutes, and I was shocked. In these 9 minutes, a sufferer talks about her experience: that she was lied to by the FDA, by the companies, by the government. Because none of those who had suffered side effects had even received any form of medical help. They try to pass off these effects, not to take them seriously or to trivialize them. At the end, she tearfully reads out the suicide note of a friend who had developed autoimmune problems and taken her own life because of it. The decisive factor, apart from her suffering, was probably her powerlessness in the face of the total silence and the walls of the political system in the USA.
Are things different in other countries? Will the damage attributable to vaccinations be recognized as such, say in Germany? Or will it be another years-long legal battle, as in other cases? We will see. I had pointed out earlier: behind closed doors, one hears about such cases. I also read about a case where a patient was referred to the hospital, where he was not seen as a potential case of vaccine side effects, and was dismissed.
The other day I was talking to a colleague. He told me about a doctor in whose practice an elderly woman collapsed dead immediately after a vaccination. The doctor did not report this as a vaccination side effect. That’s a big hassle, costs time and, stupidly, maybe even reputation. Another colleague told me similar things: colleagues who see very clearly that side effects occur, but do not report them. Therefore, we can assume that the number of unreported cases is very high, and that the numbers published in the studies so far or that can be taken from the side effect databases are grossly underestimated. This is also the reason why people who experience such side effects should definitely file a report. In Germany, you can do this yourself on the pages of the Paul Ehrlich Institute.
More deaths among vaccinated than non-vaccinated in England
An analysis carried out by Prof Fenton, a mathematician and risk analysis specialist at Queen Mary University in London, is available as a pre-publication. He has compared the age-standardised mortality of the vaccinated with that of the unvaccinated, using publicly available data from Public Health England and the Office of National Statistics up to week 26 (July 2nd, 2021). Looking at this data, we see that the age-standardized deaths per 100,000 population, regardless of cause, is lower in the unvaccinated group (25.3) than in the once-vaccinated group (89.3), but higher than in the twice-vaccinated group (14.7). Age standardization leads to the inclusion of the effect that in the UK, about 75% of the population for whom vaccination is approved is now vaccinated. However, the authors point out that national statistics are missing data on about 10 million citizens. The unstandardized mortality rates of 8.99 (once vaccinated) and 25.5 (twice vaccinated) are much higher than for the unvaccinated (4.57). The authors note that death rates from Covid-19 are low overall, accounting for just 1.6% of all deaths. They also believe that the statistics are not reliable because so much data is missing and there are such large discrepancies. The authorities have promised better statistics in three weeks. So one can be curious.
And in Germany? The RKI mortality figures on Covid-19 deaths
I would like to see similar statistics in Germany. The Federal Statistical Office has not even managed to publish mortality figures for 2020, let alone provisional figures for 2021 and let alone breakdowns by vaccinated and unvaccinated against SARS-CoV2. Therefore, one has to be a bit more indirect in Germany if one wants to know whether vaccinations have an effect and if so, what effect. I therefore looked at the mortality figures that the RKI published on Covid-19 on 28.10.2021.
If we graph all cases here by age group separately over the two years 2020 and 2021, we get the following graph (Fig. 1; I have combined men and women here because I have seen that the sexes do not differ much from each other and because I am interested in the overall trend; the RKI table contains numerical values “smaller than 4”; I have included these as 3.99 in the calculation; this has a conservative effect):
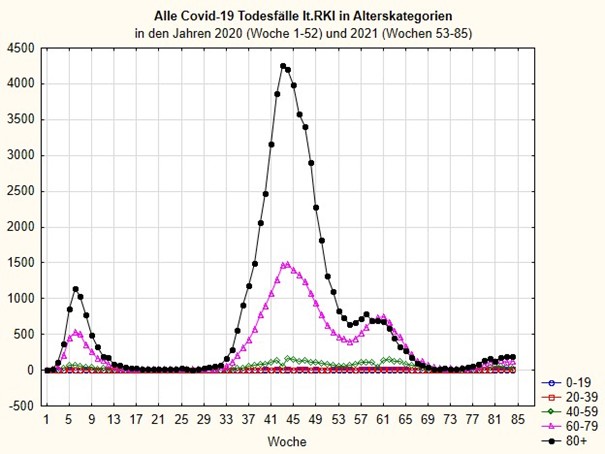
You can see from this figure: towards the end of 2020 there was a sharp increase in mortality, especially among the old (over 60 and 80 years old). Now, towards the end of 2021, there is actually not nearly as much of a problem as one might infer from the media claptrap. Actually, if the effectiveness of the vaccination is as good as one thinks, the magic should now be over for good. How did Mrs Merkel oracle? The pandemic is over when a vaccination is found. It has been found. It has been given to a large part of the population. Since the herd immunity for any infection is 1-1/R, and R, the reproductive number of the virus was between 2 and 3, it follows that 50-66% of the population must be either immune or immunized [3]. This number should have been reached long ago with all the vaccinations and positive cases, not to mention the forgotten cross-immunities [4-6]. So why are we seeing this increase? Does it have to do with vaccine breakthroughs? With the fact that the vaccinated are in reality not immune, as studies from the summer already suggest [7]?
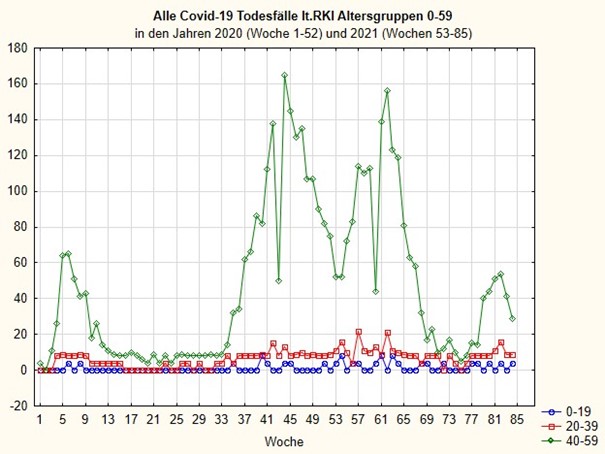
If you break down the graph above more finely by omitting the 60-79 and 80+ age groups, you get Figure 2, which makes it easier to track the trend in younger people, in this case the 40-59 age group. Let’s remember: at the beginning of 2021, i.e. in the weeks from 53, the vaccination campaign started. While the trend for the very old (Fig. 1, black curve) drops off from week 58 and for 60-79 year olds from week 61 (Fig. 1, purple curve), it only goes down for 40-59 year olds after week 63 and is now rising again for this age group.
If we break down Figure 2 even further to better capture the trend in the youngest age categories, we get Figure 3. The first thing we see is that there were very few Covid 19 deaths in these young age categories in 2020. The jumps to “4” in the very young children and adolescents are artefacts. Because here the RKI marked “less than 4” and I set this number to 3.99 to be able to show the curves. But it could also be one, two or three. So the first thing you see is that children, adolescents and young adults are so few among the Covid 19 deaths that it is medical nonsense to want to give a vaccination to this age group, especially since we know that the vaccination does not protect against infection and transmission of the virus [7-9]. What I find much more worrying is that Covid-19 mortality has been rising in these age groups since the vaccination campaign began. If you ignore all the frequencies of “4” because they may be an artefact and just visually average all the values above 4 in weeks 1-52 and do the same for weeks 53 to 85, you can see immediately: something is wrong here.
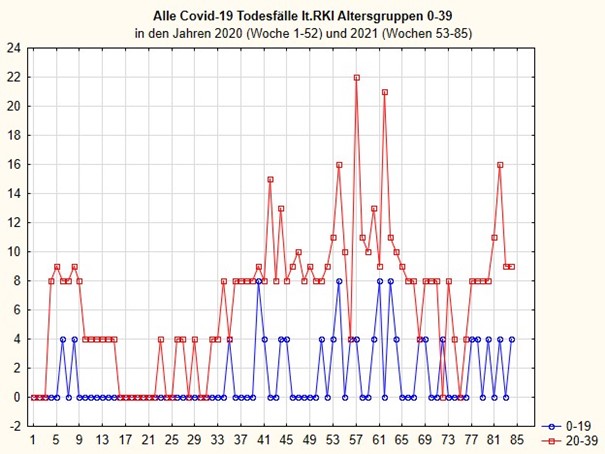
While in the overall trend (Fig. 1) Covid 19 mortality rates are decreasing in 2021, they are increasing in the age groups of children, adolescents and adults, even though there has been no more wave of infection and, according to theory, vaccination should protect.
If you can’t believe your eyes, you can see this here by looking at the summary over 2020 and 2021 for the two age groups separately in boxplots that include the robust medians and the data range. Even a blind man can see that these differences are statistically significant. And I say it again: the data contain artefacts that have a conservative effect because the RKI did not resolve death counts below 4. So here are the boxplots in Figures 4 and 5.
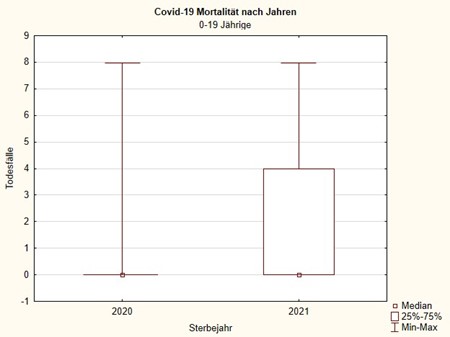
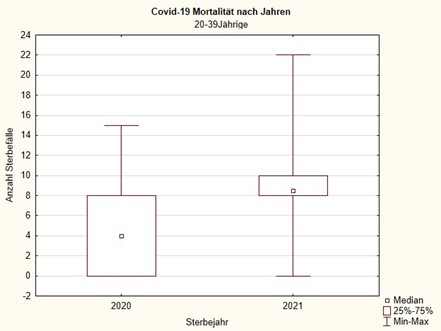
I think these two statistical graphs look alarming, especially since we were not dealing with a major SARS-CoV2 wave in 2021, at least not yet. Moreover, the year 2021 is not yet over and thus the data basis for this summary is smaller, which also exerts a conservative effect. The interpretation that these figures conceal deaths that are directly or indirectly related to the SARS-CoV2 vaccination is obvious. To really be able to confirm this or rule this out with greater certainty, we would now need to compare exactly the age-standardized mortality figures of the years before with those of 2021 and ideally have a breakdown by vaccination status. Then we would know. Does anyone among those responsible really want to know? If so, then the “Statistische Bundesamt” (federal statistical office) should be instructed to provide exactly these figures as a matter of urgency. If this does not happen, we can either assume that we live in a banana republic or that nobody wants to know. Because what we know so far is actually enough to call off the vaccination campaign, at least among young people. It is irresponsible. And the data from the RKI show this very clearly in my view.
All this should at least be reason enough to lift the prohibitions on thinking that prevail in this country and that lead to equating being vaccinated against SARS-CoV2 with being a “good democrat and citizen” and vaccination scepticism or hesitancy with “lateral thinking” that leads to Nazi suspicions.
I repeat myself: a Covid-19 disease is a stroke of fate; it may be possible to avoid it or mitigate it so that it does not degenerate into a drama by taking some preventive measures – such as good vitamin D levels and a healthy lifestyle. A vaccine side effect due to a poorly tested vaccine that has been whipped through the approval process is a bodily injury, sometimes resulting in death, which only loses its legal edge through informed consent. Given the current data, can anyone give informed consent at all? Actually, the state that granted the approval is liable for the consequences. At the moment, it is doing everything in its power not to take note of possible problems. The companies have taken themselves out of liability by passing it on to the state. That was smart from my point of view – in terms of their own economic interests – because they knew that they would not be able to cushion what would come their way.
What I have long called for is overdue: a careful, industry-independent, long-term observational study of a large cohort, perhaps a million, of freshly vaccinated people to really see exactly which side effects occur and how often. Only then can one make an informed decision as to whether this risk is preferable to the comparatively manageable risk of an infection with complications.
Because never before in the entire history of medicine has there been an infection whose public image and scientific data diverged as much as in the case of SARS-CoV2. Never before has a procedure as untested as mRNA or vector vaccination been rushed through emergency approval with reference to the threat. And I think: never in the post-war era have more people proverbially risked life and limb by public misjudgements in such a way that it seems easier and more consistent to perpetuate the myth of the killer virus and salvation by the vaccine injection than to encourage reflection and declare a moratorium.
What do you do in Iceland if you get lost in a forest? Asks an Icelandic joke. It’s simple: you get up and look around (because the trees there are so small). We should do something similar now: stand still, admit our mistakes, and get out. I wonder if the political and scientific actors in this tragedy have the stature to take this step?
Sources and literature
- Thacker PD. Covid-19: Researcher blows the whistle on data integrity issues in Pfizer’s vaccine trial. BMJ. 2021;375:n2635. doi: https://doi.org/10.1136/bmj.n2635.
- Angell M. The Truth About The Drug Companies: How They Deceive Us And What To Do About It New York: Random House; 2005.
- Omer SB, Yildirim I, Forman HP. Herd Immunity and Implications for SARS-CoV-2 Control. JAMA. 2020. doi: https://doi.org/10.1001/jama.2020.20892.
- Mateus J, Grifoni A, Tarke A, Sidney J, Ramirez SI, Dan JM, et al. Selective and cross-reactive SARS-CoV-2 T cell epitopes in unexposed humans. Science. 2020;370(6512):89-94. doi: https://doi.org/10.1126/science.abd3871.
- Ng KW, Faulkner N, Cornish GH, Rosa A, Harvey R, Hussain S, et al. Preexisting and de novo humoral immunity to SARS-CoV-2 in humans. Science. 2020:eabe1107. doi: https://doi.org/10.1126/science.abe1107.
- Nelde A, Bilich T, Heitmann JS, Maringer Y, Salih HR, Roerden M, et al. SARS-CoV-2-derived peptides define heterologous and COVID-19-induced T cell recognition. Nature immunology. 2021;22(1):74-85. Epub 2020/10/02. doi: https://doi.org/10.1038/s41590-020-00808-x. PubMed PMID: 32999467.
- Riemersma KK, Grogan BE, Kita-Yarbro A, Halfmann PJ, Segaloff HE, Kocharian A, et al. Shedding of Infectious SARS-CoV-2 Despite Vaccination. medRxiv. 2021:2021.07.31.21261387. doi: https://doi.org/10.1101/2021.07.31.21261387.
- Chau NVV, Ngoc NM, Nguyet LA, Quang VM, Ny NTH, Khoa DBaP, Nguyen Thanh, et al. Transmission of SARS-CoV-2 Delta Variant Among Vaccinated Healthcare Workers, Vietnam. SSRN Preprints. 2021. doi: http://dx.doi.org/10.2139/ssrn.3897733
- Gazit S, Shlezinger R, Perez G, Lotan R, Peretz A, Ben-Tov A, et al. Comparing SARS-CoV-2 natural immunity to vaccine-induced immunity: reinfections versus breakthrough infections. medRxiv. 2021:2021.08.24.21262415. doi: https://doi.org/10.1101/2021.08.24.21262415.